26 Lens Management
26.1 Phaco-Vitrectomy
26.2 Pars Plana Lensectomy
26.3 Intraocular Lens Explantation
26.4 Secondary Intraocular Lens Insertion Clinical Scenarios & Clinical Decision Making
26.5 Sulcus Intraocular Lens
26.6 Anterior Chamber Intraocular Lens
26.7 Iris Fixated Intraocular Lenses
26.8.1 Scleral Sutured Intraocular Lens – Traditional 2 Point Fixation
26.8.2 Scleral Sutured Posterior Chamber Intraocular Lens 4 Point Fixation
26.8.3 Scleral Sutured Posterior Chamber Intraocular Lens – “Hoffman” Corneoscleral Pockets
26.8.4 Alternate Technique to Rescue a Dislocated IOL – Triangular Scleral Flap, Sutured IOL Technique
26.8.5 Suturing Without Exchanging the Intraocular Lens
26.9 Sutureless Scleral Fixation of an Intraocular Lens
26.3 Intraocular Lens Explantation
An intraocular lens (IOL) may need to be re-positioned or removed if it:
- Is subluxed or dislocated (Figure 26.3.1)
- Is of incorrect power
- Is defective (e.g. opacified)
- Is harboring a potential biofilm in a chronically infected eye (e.g. Propionibacterium acnes)
- Is causing persistent inflammation as in eyes with anterior loop PVR
- Is rubbing on the iris as in eyes with Uveitis-Glaucoma-Hyphema (UGH) Syndrome
In some cases, subluxed sulcus IOLs without vitreous prolapse may be repositioned without vitrectomy. However, dislocated IOLs or those requiring suturing often require vitrectomy. An IOL that has dislocated posteriorly will need to be retrieved from the retinal surface. IOLs which are defective or of incorrect power may require vitrectomy if they have become fibrosed to the capsular bag and require explantation in toto.

1. Vitrectomy
Perform a pars plana vitrectomy, removing any remaining lens material in the capsule or on the retina. Sclerotomies should be positioned keeping in mind the need for corneal or scleral wounds to remove or introduce IOLs, and the placement of a secondary scleral-fixated or sutured intraocular lens (if this is planned). The posterior hyaloid should be elevated if a PVD is not present. Perform a thorough peripheral depressed examination to exclude pathology requiring treatment and perform a depressed peripheral shave in areas of scleral sutures, if planned.
2. Determine
- The type of IOL.
- If there is sufficient support for sulcus placement of the IOL.
A) If the lens is a foldable one-piece it will need to be removed. One-piece lenses are too small and pliable to be successfully sutured to sclera and frequently cause UGH syndrome if sulcus placement is attempted. The size of the wound may be kept relatively small (e.g. 3mm) if the lens can be folded (or cut) in the anterior chamber prior to explantation. Often, one piece lenses are highly pliable and will deform and mold to a small corneal wound, although cutting the IOL or “PACMANing” it (cutting it almost all the way through and allowing the two halves to open up in a “PACMAN” shape allow for a smaller wound. Use dispersive viscoelastic to protect the cornea from excessive anterior chamber manipulation on a lens.
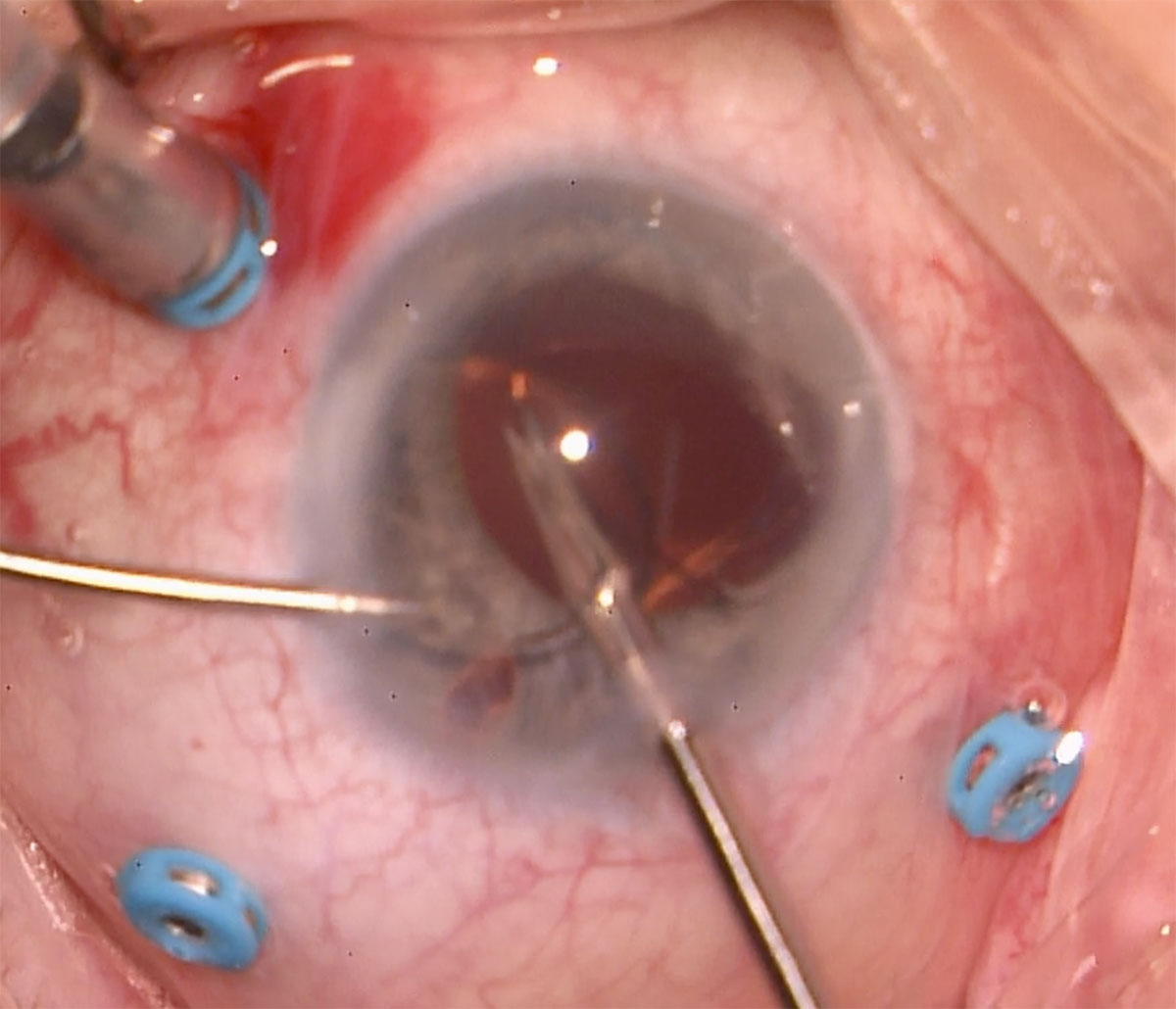
B) If the lens is a 3-piece, it may be fixated. First, check to see if there is any lens capsule remaining for sulcus placement of the IOL. If not, and the lens is still intact, it can be fixated to sclera. This avoids having to create large corneal or scleral wounds for removal of the PC-IOL and insertion of a new one. Any cortical or capsular material adherent to the PC-IOL should be removed with the vitreous cutter. If removal is necessary, most 3-pieces need to be pulled out of a large wound such as a scleral tunnel or if removed from clear cornea need to be cut with Parker/Chang forceps and then removed with a “PACMAN” technique (Figure 26.3.2). A third option for removal is to fold the lens with a cyclodialysis spatula and Duckworth IOL folding forceps in the anterior chamber then remove it through a clear corneal incision folded.
3. Create a Paracentesis and a Main Wound (Clear Corneal Incision or Scleral Tunnel) if the IOL will be Exchanged.
If a scleral tunnel is planned it can helpful to pre-place the scleral tunnel prior to vitrectomy when the globe is firmer but defer entering the anterior chamber until ready for IOL removal. Ensure the wound is large enough for the IOL (whether it is to be removed in toto or cut).
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.