11 Rhegmatogenous Retinal Detachment – Scleral Buckle
11.3 Removal of Scleral Buckle Implant
A scleral buckle may need to be removed for the following reasons:
- Extrusion
- Infection and/or endophthalmitis (extremely rare)
- Intractable diplopia
- Pain
- MIRAgel episcleral implant swelling
Most cases of scleral buckle removal are performed for extruding buckles. Closing the conjunctiva over an extruded buckle usually results in future re-extrusion, so it is often best just to remove it. It is usually safe to do so three months or later after implantation, when the retina will have been re-attached and the buckle indent will surprisingly remain even after buckle removal. If the buckle has been in situ for many years, it is important to carefully examine the peripheral retina with indirect ophthalmoscopy for signs of intrusion, which risks resulting in a perforated globe when the scleral buckle is removed. It is always useful to have a scleral patch graft available in case this occurs.
The MIRAgel implant (MIRA, Inc.) was a hydrogel material used for scleral buckling that was introduced in the 1980s. It had the advantage of being a sponge-like substance with hydrophilic pores that could hold anti-infective agents when soaked in them. The implants were also known to increase in size after their surgical implantation. This swelling caused long term complications after 5-10 years of implantation when it would cause an orbital mass effect, extraocular motility disorders, scleral thinning and implant migration and exposure (Figure 11.3.2). Sometimes the mass effect was misdiagnosed as an orbital tumor. The product was discontinued in 1995. MIRAgel implants are particularly challenging to remove because of their brittle nature.
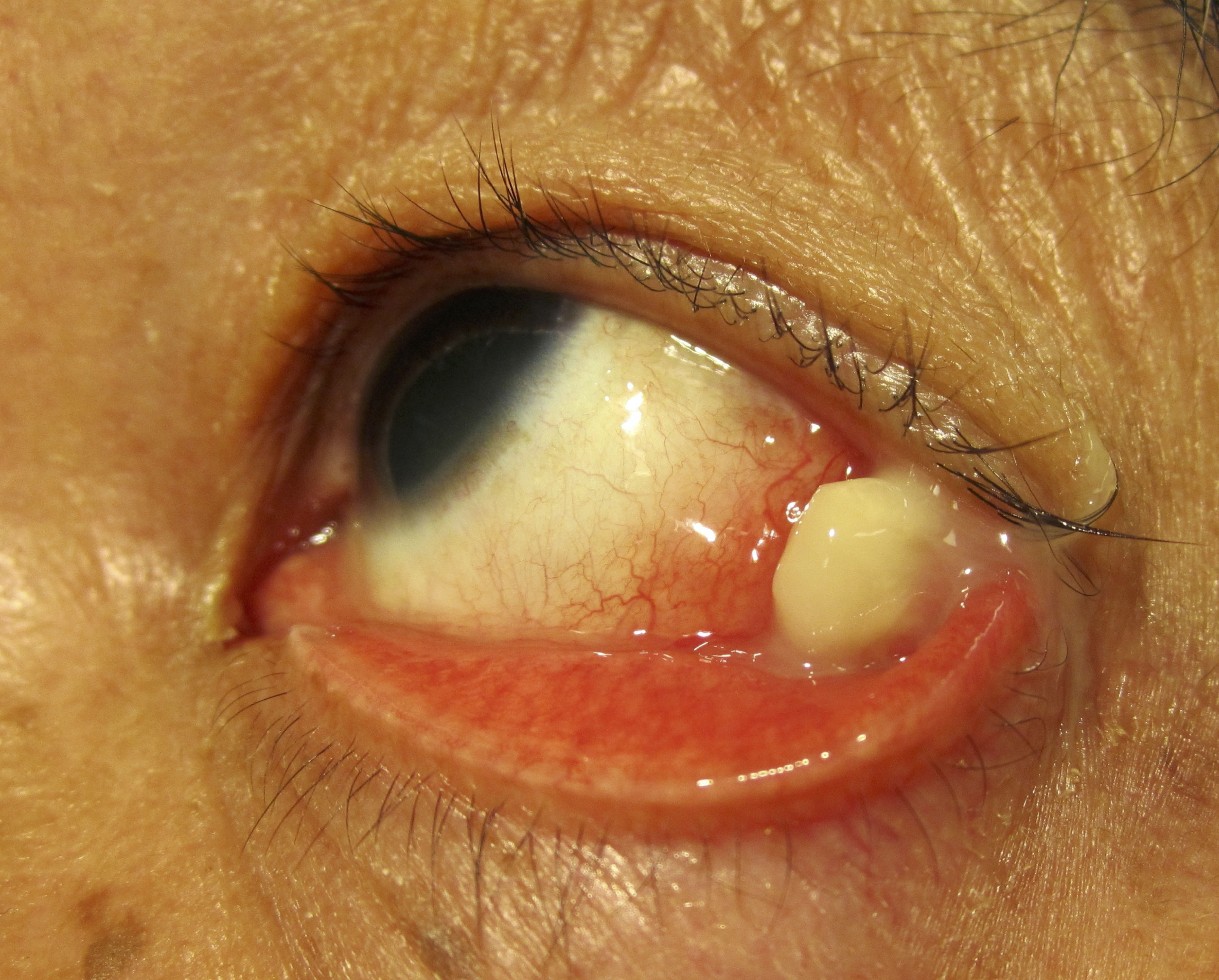
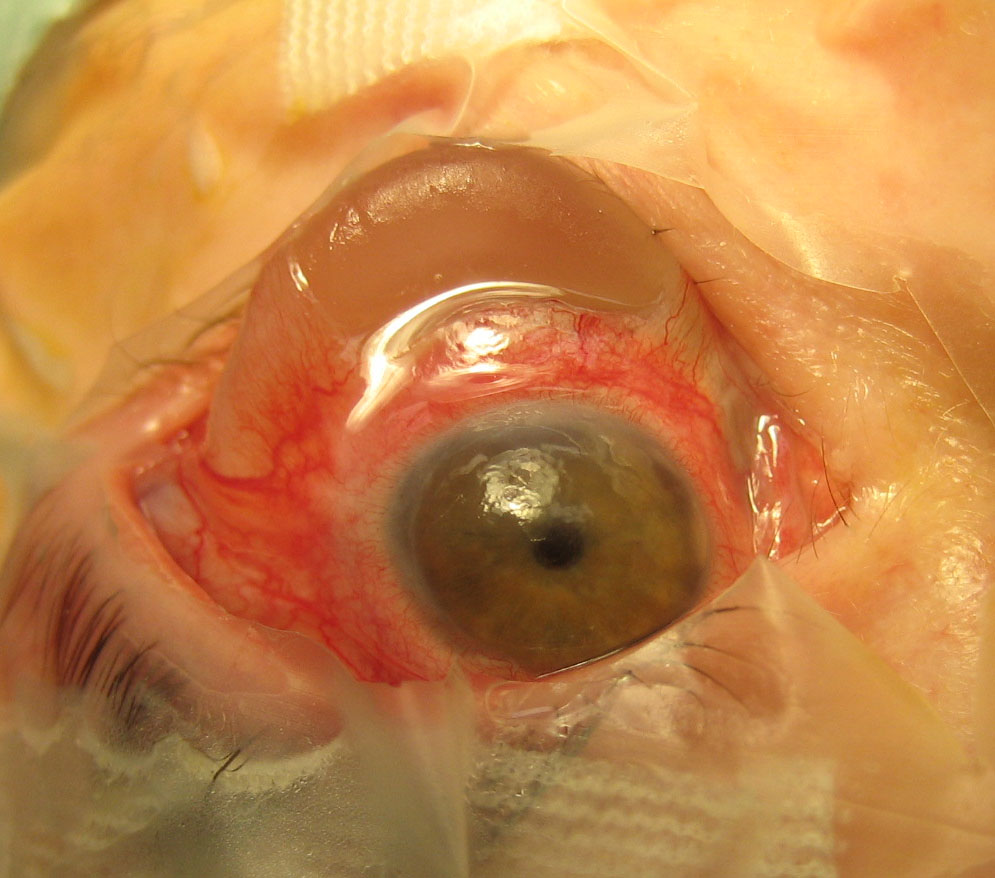
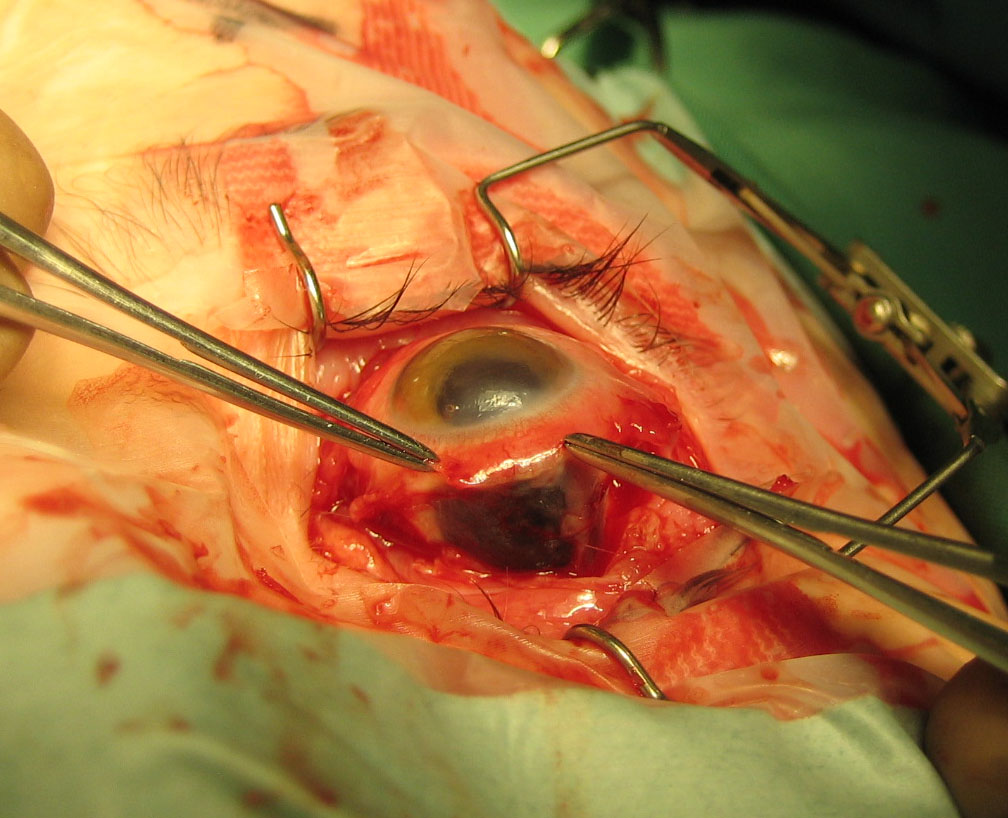
Figure 11.3.3 Following Removal of Implant in Figure 11.3.2 the Sclera was Found to be Extremely Thin
- Conjunctival forceps
- Westcott scissors
- Stevens tenotomy scissors
- Cotton-tips (q-tips)
- Muscle hooks (e.g. Jameson and fenestrated)
- Traction sutures
- Indirect ophthalmoscope and condensing lens
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.