26 Lens Management
26.1 Phaco-Vitrectomy
26.2 Pars Plana Lensectomy
26.3 Intraocular Lens Explantation
26.4 Secondary Intraocular Lens Insertion Clinical Scenarios & Clinical Decision Making
26.5 Sulcus Intraocular Lens
26.6 Anterior Chamber Intraocular Lens
26.7 Iris Fixated Intraocular Lenses
26.8.1 Scleral Sutured Intraocular Lens – Traditional 2 Point Fixation
26.8.2 Scleral Sutured Posterior Chamber Intraocular Lens 4 Point Fixation
26.8.3 Scleral Sutured Posterior Chamber Intraocular Lens – “Hoffman” Corneoscleral Pockets
26.8.4 Alternate Technique to Rescue a Dislocated IOL – Triangular Scleral Flap, Sutured IOL Technique
26.8.5 Suturing Without Exchanging the Intraocular Lens
26.9 Sutureless Scleral Fixation of an Intraocular Lens
26.8.3 Scleral Sutured Posterior Chamber Intraocular Lens – “Hoffman” Corneoscleral Pockets
An alternate method to scleral flaps for sutured posterior chamber intraocular lens (PC-IOL) is to secure the IOL via scleral pockets initiated in the cornea near the limbus, utilising a corneoscleral (“Hoffman) pocket technique. The advantages of this method is that conjunctival peritomy and scleral cautery is not required, it can be performed even if the conjunctiva is scarred down, the suture knot is buried without the need for knot rotation and the scleral pocket itself is self closing.
The Hoffman pocket technique can be used to sclerally fixate a new PC-IOL or to rescue an existing subluxed or dislocated PC-IOL. It is particularly useful for a subluxed lens-bag complex with a capsular tension ring in situ.
Begin by marking the horizontal meridian of two corneo-scleral (“Hoffman”) pockets located 180º apart (Figure 26.8.3.1). An incision (using either a 15 degree, guarded diamond or beaver blade) of approximately 30º in width and 300 – 400 µm depth (half scleral thickness) is created on either side (Figure 26.8.3.2).
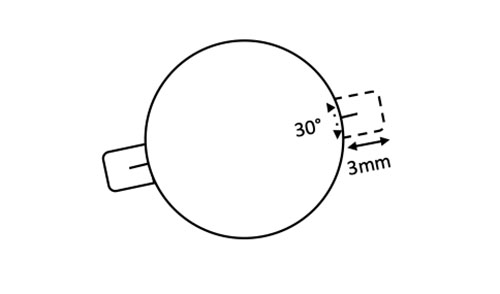
The scleral pockets are dissected posteriorly towards the fornix using a crescent blade, aiming for a pocket length of 3.0 mm (Figure 26.8.3.3).
Fill the anterior chamber with viscoelastic via a paracentesis.
A. If the Patient is Aphakic (or a Dislocated IOL Has Just Been Removed)
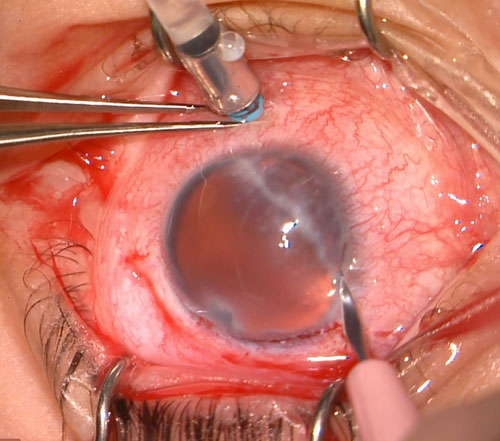
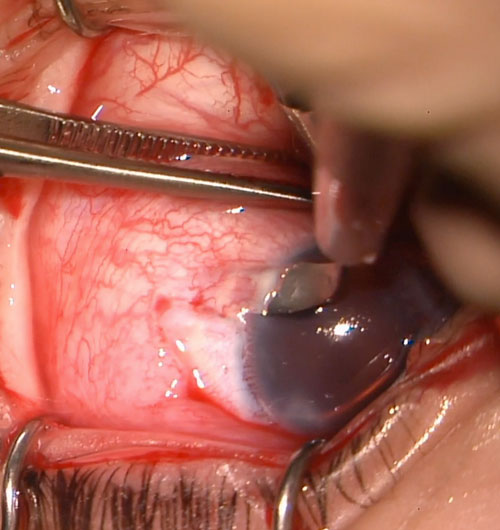
Pass a CV-8 Gore-Tex suture ab-externo through the wall of the eye 2-3mm posterior to the limbus in the location of the corneo-scleral (“Hoffman”) pocket (Figure 26.8.3.4). Externalize the suture through a main wound (keeping the needle on the suture) then loop it through the eyelets of an IOL (Figure 26.8.3.5 and Figure 26.8.3.6). Pass the needle back through the main wound. Insert a bent 27-gauge needle through the corneo-scleral (“Hoffman”) pocket just above the initial entry point. Dock the needle of the Gore-Tex suture into the 27-gauge needle and use this to externalise the suture from the eye (Figure 26.8.3.6). Repeat on the process on the other side (Figure 26.8.3.7).
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.