13 Rhegmatogenous Retinal Detachment Special Scenarios
13.1 Rhegmatogenous Retinal Detachment: Re-detachment Surgery
13.2 Macular Hole Retinal Detachment
13.3 Retinoschisis Retinal Detachment
13.4 Optic Disc Pit Retinal Detachment and Maculopathy
13.5 Giant Retinal Tear Detachment
13.6 Retinal Dialysis
13.7 Macular Folds
13.8 Sickle Cell Detachment
13.9 Viral Retinitis Associated Retinal Detachment
13.10 Paediatric Retinal Detachment
13.11 Coloboma Associated Retinal Detachment
13.12 Inherited Retinal Dystrophies and Retinal Detachment
13.5 Giant Retinal Tear Detachment
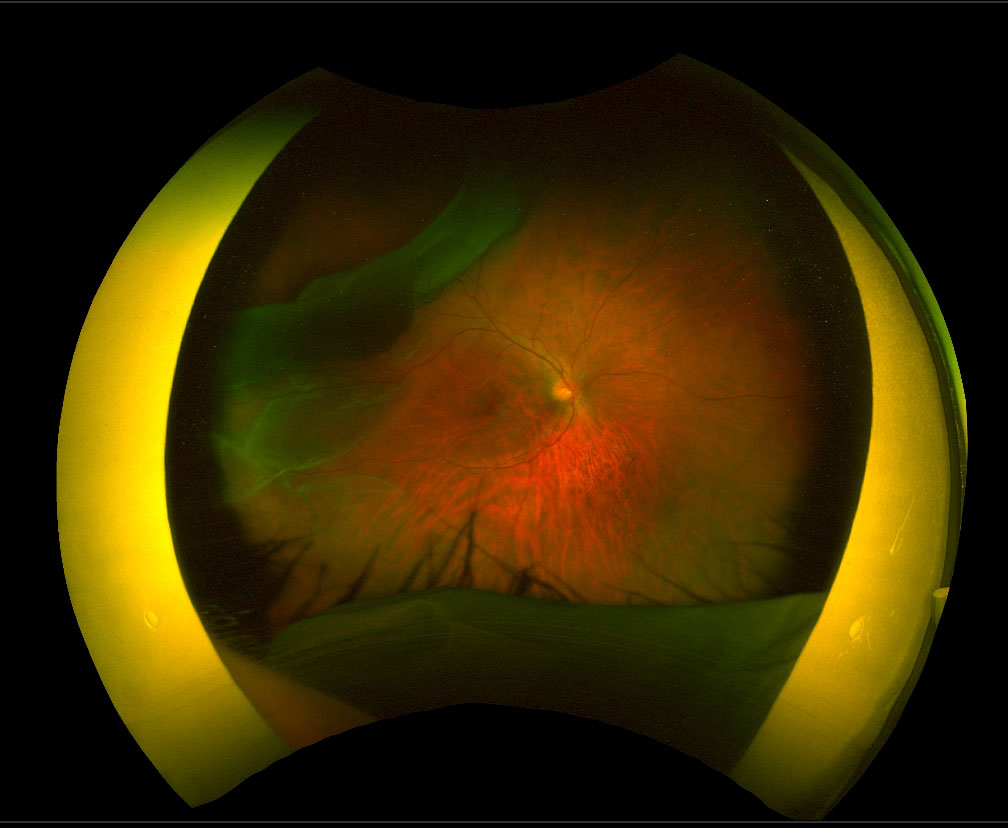
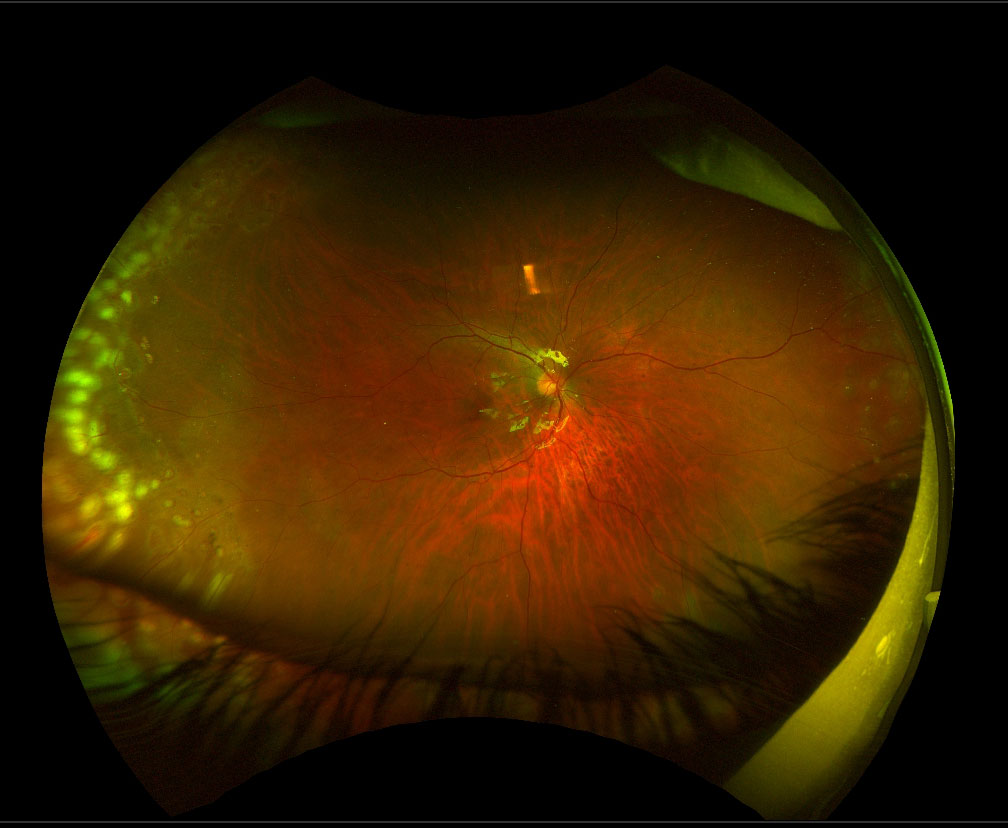
Management of a retinal detachment associated with a giant retinal tear (GRT, greater than 3 clock-hours) is more difficult than repair of a regular rhegmatogenous retinal detachment for the following reasons:
- The retinal detachment is usually large, bullous and mobile (Figure 13.5.1 and Figure 13.5.4)
- Vitreous traction at the anterior margins of the tear
- Risk of slippage of the retina
- Risk of retinal folds through the macula
- Risk of subretinal perfluoro-n-octane (PFO) or silicone oil
- Risk of proliferative vitreoretinopathy (PVR)


The infusion cannula should be placed away from the detachment (to avoid hitting the bullous retina or subretinal placement) and the inflow directed away from the GRT.
Key to successfully operating on GRT retinal detachments is meticulous relief of vitreo-retinal traction, particularly at the horns and anterior edge of the tear (Figure 13.5.5A). The anterior flap of retina can be excised as it is non-functional and will only induce PVR.
A. Core Vitrectomy
May be challenging due to the high mobility of the retina. If the retina is very mobile and vitrectomy is deemed unsafe, it may be advantageous to inject intravitreal PFO to flatten the posterior retina and stabilize the anterior retina for further vitrectomy. This also assists in peeling of any anterior PVR membranes. Make sure that the posterior hyaloid is detached before injecting PFO to avoid trapping a sheet of vitreous underneath it. Furthermore, avoid instilling the PFO beyond any breaks until traction has been removed, otherwise there is increased risk of subretinal PFO.
B. Peripheral Vitrectomy
Peripheral vitrectomy may be assisted by scleral indentation. If PFO was used to stabilize the retina, caution should be taken during scleral depression in order to avoid migration of PFO to the subretinal space. In some cases the crystalline lens may need to be sacrificed (lensectomy) in order to facilitate complete clearance of the anterior vitreous.[1] In such cases it is preferable to retain the posterior capsule to prevent the endotamponade migrating into the anterior chamber and for future sulcus placement of an intraocular lens.
Verstraeten T, Williams GA, Chang S, et al. Lens-sparing Vitrectomy with Perfluorocarbon Liquid for the Primary Treatment of Giant Retinal Tears. Ophthalmology. 1995. doi:10.1016/S0161-6420(95)31063-9
C. Scleral Buckling
Scleral buckling may be required, particularly if PVR is present. A circumferential wide buckle positioned on the vitreous base in an attempt to maximize the relief of traction.[2] If a combined procedure is planned, the scleral buckle should be positioned first in an attempt to minimize retinal manipulation after re-attachment. Scleral buckling has the disadvantage of increasing the risk of retinal slippage though this is infrequent if the buckle is slightly released during the FAX. Consider a scleral buckle in those patients with inferior or phakic GRT.
Goezinne F, LA Heij EC, Berendschot TTJM, et al. Low redetachment rate due to encircling scleral buckle in giant retinal tears treated with vitrectomy and silicone oil. Retina. 2008;28(3):485-492. doi:10.1097/IAE.0b013e318150d879
Endodiathermy is used to demarcate the horns of the tear. Intravitreal PFO is injected up to the posterior edge of the GRT to flatten the retina. The eye should be rotated in the opposite direction from the tear to minimize the development of retinal folds or sub-retinal PFO.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.