2.2 Vitrectomy Machines & Setup
Many different vitrectomy machines are available, each with their advantages and disadvantages. Trainees should familiarize themselves with as many different units as possible. A number of commonly used machines will be discussed throughout this chapter.
Maximum cut-rates vary with the machine and hand-piece being used. Standard cut- rates have slowly increased over time to 10000-20000cpm. This has been possible through the use of dual pneumatic instead of spring-based mechanisms. Recently, the cutter design has been modified from cutting in only one direction to two-directional cutters, which allow for vitreous cutting to occur twice, resulting in effectively greater cut rates and duty cycle. Higher cut-rates reduce the pressure variation across the port with each port-opening cycle, allowing for greater fluidic stability around the vitrectomy port which may cause less iatrogenic traction and tears. The vitreous cutter can be placed closer to the retinal surface with safety; this is especially important when cutting near mobile retina or dissecting membranes close to the retinal surface. A higher cut-rate also reduces surgical time.
The vacuum should be set such that it is low enough for safe vitrectomy while being high enough for adequate removal of vitreous. Excessively high vacuums induce unnecessary vitreo-retinal traction, especially with two-directional cutters. High vacuums (650mmHg) are useful when cutting in the mid-vitreous for efficient remove of vitreous as well as induction of posterior vitreous detachments. As one approaches the retina, lower vacuum reduces traction on the retina. Different vacuum settings on the machine can be utilized depending on the stage of the case.
Duty Cycle:
- Duty cycle refers to the percentage of open port time for each complete cut cycle
Proportional vs “3D”
In “proportional” vitrectomy the cut-rate remains constant, whilst the vacuum is controlled by the foot treadle. In “3D” (Dual Dynamic Drive) vitrectomy both the cut rate and vacuum are controlled by the foot pedal. These are customizable and often inversely related (i.e. as the vacuum increases the cut rate decreases). With the improved vitrectomy probes with improved duty cycle, proportional vitrectomy that has a fixed high cute rate but variable vacuum is the most useful setting.
A plethora of hand-pieces are currently available. The greatest distinctions within each brand are the style of cutter (guillotine or rotary) and gauge of instrument. 20, 23, 25 and 27-gauge instruments are all used world-wide. The main differences between 20-gauge and 23-, 25-, and 27- (“microincisional”) gauge instruments are shown below:
Larger Gauge
Stiffer instruments
Longer instruments (useful in high myopes)
Faster silicone oil insertion / removal
Fragmentation handpiece requires a 20- or 23- gauge sclerotomy
Smaller Gauge
Often sutureless (faster surgical times)
Less vitreous traction
Valved cannulae provide less risk of vitreous incarceration at the ports and greater IOP control
Smaller selection of instruments in certain gauges (i.e. no illuminated endolaser in 27-gauge)
Microincisional vitrectomy surgery (MIVS) has now become standard, with 20-gauge vitrectomy being rarely performed.
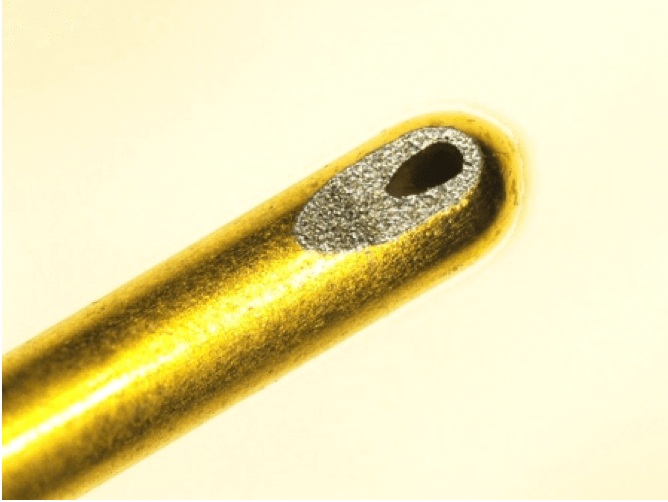
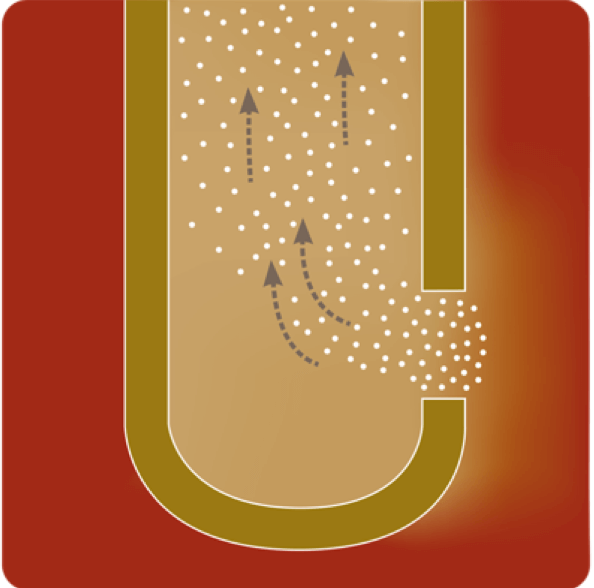
In 2017, Bausch + Lomb introduced the Vitesse® hypersonic vitrectomy instrument for its Stellaris Elite vitrectomy machine. In contrast to guillotine-based systems that use a second inner needle to cut aspirated vitreous strands inside of the vitrector port, the hypersonic system consists of a single-bore 23-gauge vitrectomy probe that liquifies the vitreous immediately in front of the port prior to aspiration (Figure 2.2.1 and Figure 2.2.2). This effect is achieved through high frequency needle tip oscillation that allows the port to remain open at all times with a 100% duty cycle. The hypersonic liquefaction of vitreous may decrease iatrogenic traction on the retina and result in greater flow stability. In contrast to guillotine cutters, the hypersonic vitrectomy instrument has a smaller port opening (Figure 2.2.3) and can also have variations in shape and location which may result in unique probe designs in the future.

Contact viewing systems employ a contact lens placed on the cornea, such as the Volk MiniQuad XL (Figure 2.2.4) and Ocular Landers lens. These often require a skilled assistant to hold the lens but give excellent visualization of the retinal periphery. Non-contact viewing systems include the Oculus BIOM series (Figure 2.2.5), Carl Zeiss Meditech RESIGHT (Figure 2.2.6), Volk Merlin, Ocular Landers, Opto Global FlexMax and Haag-Streit EIBOS. These give the surgeon freedom to operate without an assistant but require greater rotation of the eye to view the periphery, and the field of view tends to be 10 degrees less than with a contact viewing system.
Flat (plano) contact lenses can be used with a sterile operative hydroxypropyl methylcellulose- based solution or Viscoelastic to provide enhanced visualization of the posterior pole for macular work. The RESIGHT and EIBOS systems have a magnified lens (“green lens”) that does not offer as much stereopsis as a contact lens but does allow for a greater field of view (especially useful in diabetic cases).
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.