19.1 Vitreous Biopsy
Vitreous biopsies may be:
- Diagnostic to determine the etiology of vitritis such as suspected:
- Endophthalmitis (including Proprionibacterium acnes and fungal) not responding to intravitreal antibiotics
- Intraocular lymphoma
- Intravitreal amyloidosis
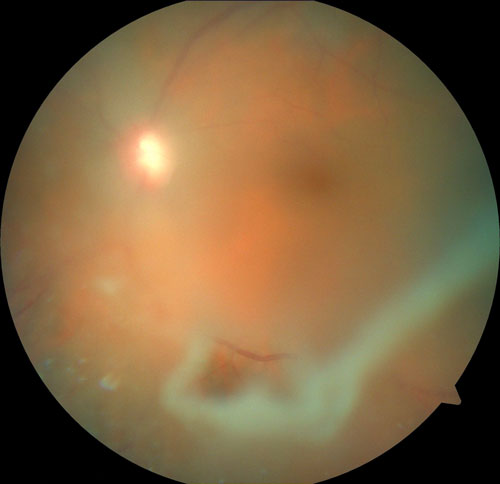
- Therapeutic to remove infectious or inflammatory material that is causing vitreous opacity (Figure 19.1.1)
- Consult with laboratory to ensure that:
- The cytologist or pathologist is prepared to deal with specimen
- Correct transport medium is used (e.g., RPMI for suspected lymphoma, Cytolyt® solution for all other non-lymphoma indications).[1] Culture plates are used for suspected infectious etiologies (aerobic and non-aerobic bacteria, viruses, fungi)
- In cases of poor posterior segment visualization, prior to the procedure perform B-scan ultrasonography to determine presence of retinal / choroidal detachment or intraocular tumors
- In cases of suspected vitreoretinal lymphoma, steroids should be stopped for 2 weeks prior to surgery, since they can cause apoptosis with lysis of lymphoma cells.[2]
Ranty ML, Laurent C, Aziza J, et al. Improving the cytological diagnosis of intraocular lymphoma from vitreous fluid. Histopathology. 2015;67(1):48-61.
Jiang T, Zhao Z, Chang Q. Evaluation of cytologic specimens obtained during experimental vitreous biopsy using B-cell lymphoma line. Eur J Ophthalmol. 2014;24(6):911-917.
There are Two Main Approaches to Vitreous Biopsy:
i. Vitreous-cutter Biopsy
- Advantages
- Obtain a larger sample with higher diagnostic yield (preferred if > 0.5cc/ml is needed); controlled operating environment with anesthesiologist present
- Disadvantages
- Reliant on operating room availability; more expensive; vitrectomy is caractogenic
ii. Fine Needle Aspiration Biopsy
- Advantages
- Can be done in clinic with local anesthesia; less expensive
- Disadvantages
- Smaller sample size with lower diagnostic yield
A vitreous sample should be obtained without diluting/contaminating it with BSS® infusion.
1. Opening
Set up for a standard three port pars plana vitrectomy but do not open the infusion line. 25 or 27 gauge cannulas with beveled insertion is preferable for self-sealing wounds. If there is poor view, consider using a 6 mm length infusion cannula to ensure the infusion is in the vitreous cavity, especially if there is coexisting choroidal or retinal detachment detected on preoperative B-scan ultrasound.
2. Prime the Cutter with Air
This ensures that any sample will not be diluted by BSS® coming from the infusion. If using the Alcon CONSTELLATION® vision system: The "Setup" screen is divided into 6 boxes. The top middle box says "Probe." In this box it says "Skip Prime". Push the button next to this and it will place a green check next to it. When everything on the machine is set up and ready to prime, just select "Start Prime" as normal. The whole system will prime like normal except there will be no fluid in the cutter line, allowing for a pure sample to be taken.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.