5.3 Oil Retention Sutures
Complex retinal detachments, such as those after open globe injuries, often require silicone oil tamponade. In eyes with traumatic or surgical aphakia and an intact iris, an inferior peripheral iridectomy effectively keeps oil out of the anterior chamber. However, eyes with aphakia and aniridia represent a particular challenge. The lack of the lens-iris diaphragm is a relative contraindication to placement of silicone oil due to the risk of anterior migration of oil leading to elevated intraocular pressure (IOP), band keratopathy, bullous keratopathy and/or complete corneal decompensation, in addition to suboptimal tamponade. First described in 2010, silicone oil retention sutures can be placed just behind the limbus to prevent oil migration in these eyes[1], and they have been shown to successfully keep oil posteriorly in a number of reports.[1,2,3,4,5,6] It is important to understand that sufficient aqueous production is essential for this technique to work, as it is ineffective in cases of hypotony (IOP < ~5).
A number of suture configurations have been proposed. The most important part of any retention suture placement is that they be in the same plane in order to effectively barricade the oil. The various patterns that have been attempted include a triangular configuration, as shown in (Figure 5.3.1), hexagonal,[7] square,[1,5] and grid,[1,8] (Figure 5.3.2). In 2012, a modification was described whereby a suture is interwoven in the triangular configuration to further stabilize the plane (Figure 5.3.2).[9] All configurations have achieved successful silicone oil barricade, owing to the high surface tension of the oil.
The technique is outlined in (Figure 5.3.1 and Figure 5.3.2) and is as follows:
- Use a 10-0 prolene suture on a CIF-4 needle (slightly curved, model 788G, Ethicon, Bridgewater, New Jersey) and a five-eighths inch long 25-gauge needle on a 1 mL syringe
- Place the initial suture across the anterior chamber from sulcus to sulcus, 1 mm behind the limbus
- Retrieve the suture across the other side within the bore of a five-eighths inch long 25-gauge needle attached to a 1 mL syringe (Figure 5.3.1A). The needle can be slightly bent for better access to receive the CIF needle
- Repeat the suture passes to achieve the desired configuration. When able, orient the sutures so they are interwoven near the limbus, as shown in (Figure 5.3.1B and Figure 5.3.2)
Gentile RC, Eliott D. Silicone oil retention sutures in aphakic eyes with iris loss. Arch Ophthalmol. 2010;128(12):1596-1599. doi:10.1001/archophthalmol.2010.300
Gentile RC, Eliott D. Silicone oil retention sutures in aphakic eyes with iris loss. Arch Ophthalmol. 2010;128(12):1596-1599. doi:10.1001/archophthalmol.2010.300
De Grande V, Rosenthal K, Reibaldi M, Gentile RC. Artificial iris-intraocular lens implantation for traumatic aniridia and aphakia assisted by silicone oil retention sutures. J Cataract Refract Surg. 2012;38(11):2045-2048. doi:10.1016/j.jcrs.2012.08.043
Du W, Chen F, Zhu J, Xie Z. Application of Modified Silicone Oil Retention Sutures in Traumatic Aphakic Eyes With Iris Loss. RETINA. 2020;Publish Ahead of Print. doi:10.1097/IAE.0000000000002643
Forlini C, Forlini M, Rejdak R, et al. Simultaneous correction of post-traumatic aphakia and aniridia with the use of artificial iris and IOL implantation. Graefes Arch Clin Exp Ophthalmol. 2013;251(3):667-675. doi:10.1007/s00417-012-2254-7
Rao RC, Cohen SR, Mian SI. Silicone Oil Retention Sutures for Retinal Detachment Repair Following Traumatic Aniridia, Aphakia, and Ruptured Globe. JAMA Ophthalmol. 2015;133(9):e151433. doi:10.1001/jamaophthalmol.2015.1433
Syed R, Jusufbegovic D, Schaal S. A Needle-Free Minimally Invasive Surgical Technique for the Placement of Silicone Oil Retention Sutures. RETINA. 2016;36(5):1032–1034. doi:10.1097/IAE.0000000000000984
Wong R, Lee EJK, Shunmugam M. Novel technique for silicone oil retention suture with secondary auto capsulotomy of fibrin membrane. Eye (Lond). 2013;27(2):280-281. doi:10.1038/eye.2012.266
Gentile RC, Eliott D. Silicone oil retention sutures in aphakic eyes with iris loss. Arch Ophthalmol. 2010;128(12):1596-1599. doi:10.1001/archophthalmol.2010.300
Yüksel K, Pekel G, Alagöz N, Alagöz C, Baz Ö, Yazc AT. SILICONE OIL BARRIER SUTURES IN APHAKIC EYES WITH IRIS DEFECTS. Retina (Philadelphia, Pa). 2016;36(6):1222-1226. doi:10.1097/IAE.0000000000000856
Gentile RC, Eliott D. Modification of Silicone Oil Retention Sutures in Aphakic Eyes With Iris Loss—Reply; Arch Ophthalmol. 2012;130(9):1231-1232. doi:10.1001/archophthalmol.2012.1616
Many reports have used ultrasound biomicroscopy with the patient in the supine position to show that the retention sutures prevent anterior oil migration.[1,5,8] In addition, we and others[7] have found that in a small subset of cases, a membrane forms in the plane of the retention sutures that creates a pseudo-iris. A central opening may form naturally, or one can use a capsulorrhexis technique to clear the visual axis.
Gentile RC, Eliott D. Silicone oil retention sutures in aphakic eyes with iris loss. Arch Ophthalmol. 2010;128(12):1596-1599. doi:10.1001/archophthalmol.2010.300
Rao RC, Cohen SR, Mian SI. Silicone Oil Retention Sutures for Retinal Detachment Repair Following Traumatic Aniridia, Aphakia, and Ruptured Globe. JAMA Ophthalmol. 2015;133(9):e151433. doi:10.1001/jamaophthalmol.2015.1433
Yüksel K, Pekel G, Alagöz N, Alagöz C, Baz Ö, Yazc AT. SILICONE OIL BARRIER SUTURES IN APHAKIC EYES WITH IRIS DEFECTS. Retina (Philadelphia, Pa). 2016;36(6):1222-1226. doi:10.1097/IAE.0000000000000856
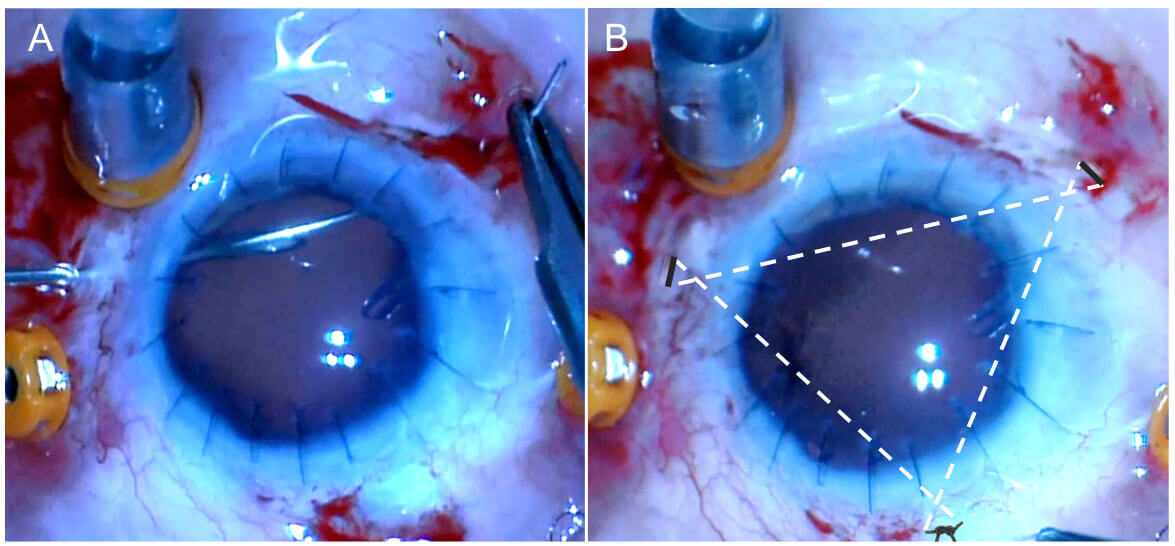
Figure 5.3.1 Oil Retention Suture Technique (Surgeon’s View, with One Point of the Triangle at 12 o’clock)
A The CIF needle (right) is passed 1mm behind the limbus across the anterior chamber in the plane of the iris. It is a received in the bore of a bent 25-gauge needle (left) on a 1cc empty syringe (not shown). B A triangular pattern is created in the plane of the iris. Note tha¬t the sutures are passed such that they cross at the points of the triangle. One knot is formed at one of the triangle points, and all points are covered with conjunctiva. The oil was successfully kept posteriorly, and the cornea remained clear. IOP was normal.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.
Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.