Chapter 17
Endophthalmitis
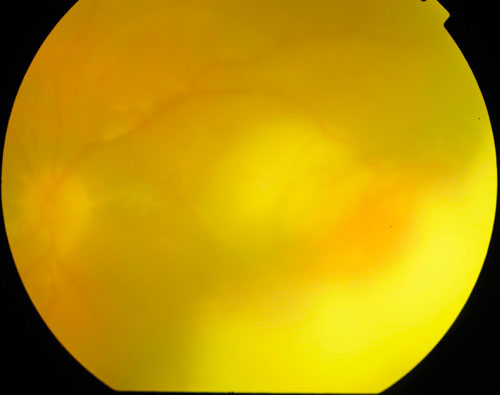
Infectious endophthalmitis (Figure 17.1) can occur secondary to hematogenous seeding (endogenous endophthalmitis) or from a variety of external insults to the eye – exogenous - (following intraocular surgery such as cataract or glaucoma surgery, trauma, or intravitreal injection). The decision to perform vitrectomy following endophthalmitis is controversial. Although the Endophthalmitis Vitrectomy Study (EVS) demonstrated better visual outcomes in patients with light perception vision or worse who underwent vitrectomy rather than vitreous tap and injection of antibiotics,[1] the EVS was conducted over 20 years ago, and many surgeons now elect to operate on different criteria. The decision to pursue vitrectomy or vitreous tap and inject depends on multiple factors including the presumed virulence of the organism, the degree of anterior segment media opacity, the availability of operating room access, and the systemic comorbidities of the patient. Advances in vitrectomy techniques and equipment, such as the development of smaller-gauge Micro-incision Vitrectomy Surgery (MIVS e.g. 23-, 25- and 27-gauge), have improved the safety of the operation.
Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study: a randomised trial of immediate vitrectomy and of intravenous antibiotics for the treatment of post- operative bacterial endophthalmitis. Arch Ophthalmol. 1995; 113(12): 1479-1496.
1. Exogenous Endophthalmitis
- Post cataract surgery
- Acute (i.e. onset within six weeks): Coagulase-negative Staphylococcus is the most common causative organism.[2] Streptococcus also occurs frequently
- Chronic (i.e. onset after six weeks): Propionibacterium acnes is the most common causative organism. Staphylococci and fungi are other causative organisms that can present in a delayed fashion[3]
- Post injection- Streptococci and Staphylococcus epidermidis are generally implicated and visual prognosis varies with worse outcomes with Streptococci.[4] Given the number of intravitreal injections, this cause of endophthalmitis is becoming increasingly common
- Post trabeculectomy/bleb- Streptococcus, haemophilus, or gram-positive organisms are the most common, and onset can occur months to years after filtering surgery[2]
- Post traumatic- Bacillus cereus, fungi and other organisms can be implicated. The visual prognosis is usually poor
Almeida DR, Miller D, Alfonso EC. Anterior chamber and vitreous concordance in endophthalmitis: implications for prophylaxis. Arch Ophthalmol. 2010;128(9):1136-1139.
Xu K, Almeida DRP, Chin EK, Mahajan VM. Delayed fungal endophthalmitis secondary to Curvularia. Am J Ophthalmol Case Rep. 2016 [in press].
2. Endogenous Endophthalmitis
Depending on the source, the range of causative organisms of endogenous endophthalmitis is wide. It includes:
- Fungal- Candida (central lines, intravenous drug use)[5]
- Gram positive bacteria
- Streptococcus (endocarditis)
- Staphylococcus aureus (cutaneous infections)
- Bacillus (intravenous drug use)
- Gram negative bacteria
- Neisseria meningitidis
- Haemophilus influenza
- Enteric organisms e.g. Escherichia Coli and Klebsiella (diabetes, urinary tract infections, liver abscess)[6,7]
Brod RD, Flynn HW Jr. Endophthalmitis: current approaches to diagnosis and therapy. Curr Opin Infect Dis. 1993;6:628–37.
Margo CE, Mames RN, Guy JR. Endogenous Klebsiella endophthalmitis. Report of two cases and review of the literature. Ophthalmology. 1994;101:1298–301.
Tseng CY, Liu PY, Shi ZY, Lau YJ, Hu BS, Shyr JM, et al. Endogenous endophthalmitis due to Escherichia coli: case report and review. Clin Infect Dis. 1996;22:1107–8.
Pros
- Improved visual outcomes in patients presenting with light perception vision or worse (EVS)[1]
- A trend (non-statistically significant) towards improved visual outcomes in diabetic patients presenting with hand motions vision or worse (EVS)[1]
- Removal of vitreous (a potential growth medium for bacteria and depot for inflammatory cytokines)[8]
- Reduction of bacterial load[9]
- Larger vitreous sample for culture[9]
- Clearance of media opacities
Cons
- Cataract formation
- Risk of retinal detachment
- Difficulties in visualization secondary to anterior segment media opacity which may lead to iatrogenic trauma
- Removal of vitreous reservoir which may reduce the half-life of future intravitreal therapy (e.g. intravitreal anti-VEGF for AMD)
- Availability of operating room access
Almeida DRP, Chin EK. Postoperative Infectious Endophthalmitis: Evolving Trends and Techniques. Practices have changed since publication of the EVS in the 1990s. Retina Today. September 2016.
Barry P, Cordoves L & Gardner S (2013) ESCRS guidelines for prevention and treatment of endophthalmitis following cataract surgery. URL https://www.escrs.org/media/uljgvpn1/english_2018_updated.pdf
Indications for Vitrectomy for Endophthalmitis Include:
- Clinical deterioration despite intravitreal antibiotics, particularly if vitreous and/or anterior chamber biopsies are equivocal
- Concomitant retained lens material or retinal detachment
- Presenting vision of light perception or worse (though this indication is extrapolated from the EVS study which only examined endophthalmitis following cataract surgery)[1]
- Endophthalmitis secondary to trauma with intraocular foreign body or penetrating eye injury
Contraindications for Vitrectomy for Endophthalmitis Include:
- Significant improvement with intravitreal antibiotics alone
- Insufficient view for safe vitrectomy
1. Anterior Chamber Washout
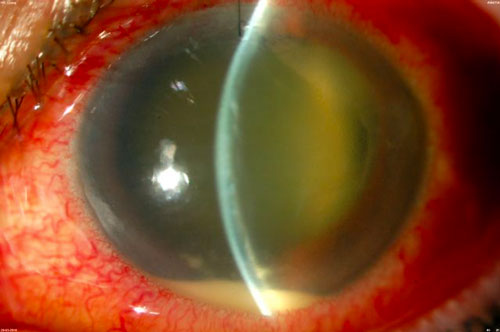
If there is significant anterior chamber hypopyon and/or fibrin which will obscure the view for vitrectomy, the anterior chamber may need to be washed out first (Figure 17.2). This is often most easily performed with the vitrector cutter through a paracentesis. A paracentesis can be made for the infusion until the view is adequate to move the infusion to the pars. Pupillary dilation with viscoelastic or iris hooks may be required if there are significant posterior synechiae and a small pupil.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.