16 Vitreomacular Interface Disorders
16.1 Epiretinal Membrane Peel
16.2.1 Macular Hole Repair (Surgical)
16.2.2 Macular Hole Repair (Medical Therapy)
16.3 Vitreomacular Traction Syndrome
16.4 Myopic Traction Maculopathy – Vitrectomy
16.5.1 Myopic Traction Maculopathy – Macular Buckling
16.5.2 Myopic Traction Maculopathy – Macular Buckling (AJL)
16.3 Vitreomacular Traction Syndrome
Vitreomacular traction syndrome (VMTS) is part of a spectrum of diseases having abnormal adhesion between the posterior hyaloid and the macula. It is characterized by incomplete posterior vitreous detachment (PVD) causing morphologic distortion of the fovea. The tractional effects of perifoveal PVD may result in complications such as tractional cystoid macular edema, retinoschisis, impending or full thickness macular hole (FTMH), foveal detachment or epiretinal membrane (ERM).[1,2] Patients with VMTS may present with gradual blurred vision, micropsia, metamorphopsia or scotoma. [3]
The International Vitreomacular Traction Study (IVTS) Group developed a classification for diseases of vitreomacular interface based on anatomic features in OCT.
- Vitreomacular adhesion (VMA): vitreous adhering to central macula without retinal morphologic changes and the attachment is within a 3 mm radius of the fovea
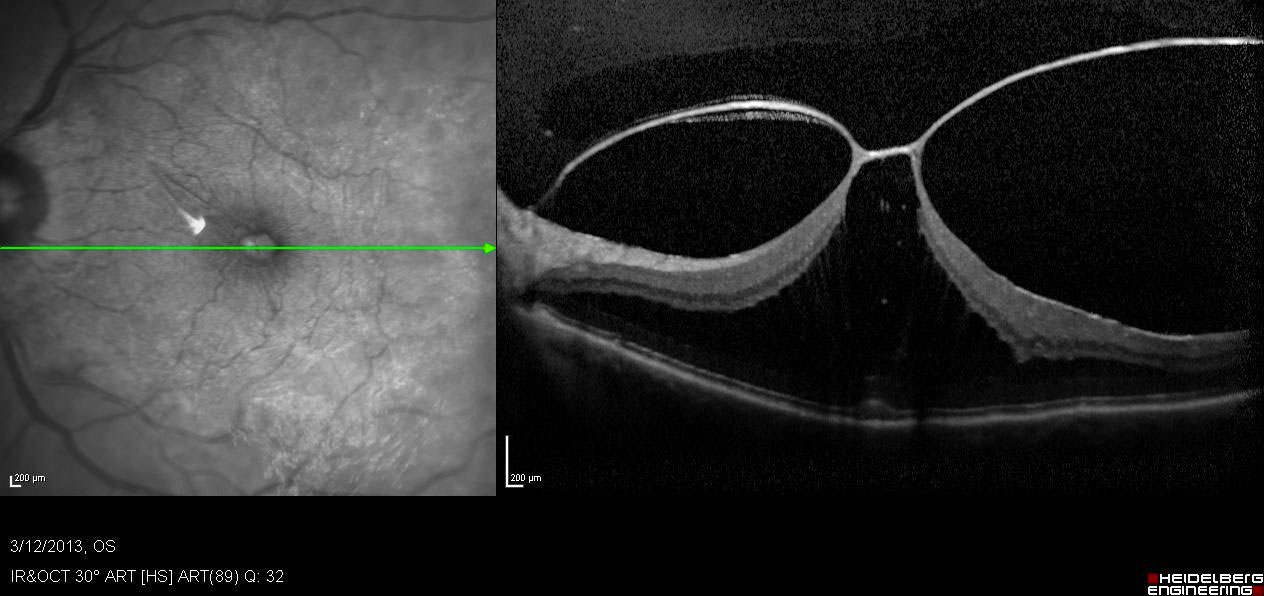
- Vitreomacular traction (VMT): vitreous adhering to central macula with anatomic changes shown by OCT, e.g. distorted foveal surface with or without elevation above the retinal pigment epithelium (RPE); intraretinal changes, but no full thickness retinal tissue dehiscence and the attachment is within a 3 mm radius of the fovea (Figure 16.3.1)
Shechtman DL, Dunbar MT. The expanding spectrum of vitreomacular traction. Optometry 2009; 80 (12): 681-687.
Bottos J, Elizalde J, Rodrigues EB, Farah M, Maia M. Classifications of vitreomacular traction syndrome: diameter vs morphology. Eye 2014; 28: 1107-1112.
Duker JS, Kaiser PK, Blinder F, de Smet MD, Gaudric A, Reichel E, Sadda SR, Sebag J, Spaide RF, Stalmans P. The international vitreomacular traction study group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology 2013; 120 (12): 2611-2619.
VMT can also be classified based on the diameter and morphology of the vitreomacular attachment.[2]
- Focal: attachment of 1500 µm or less
- Broad: attachment of more than 1500 µm
- V-shaped: perifoveal vitreous detachment with VMA
- J-shaped: incomplete PVD with temporal detachment but nasal attachment to the fovea J-shaped VMT and broad-VMT can be associated with ERM and diffuse retinal thickening, while V-shaped VMT and focal-VMT may lead to tractional cystoid macular edema and macular hole.[2]
About 20% of VMT cases may spontaneously resolve with vision improvement; 40% show long-term stability and 20% deteriorate or progress to FTMH.[4] For VMT cases which are symptomatic or progress treatment options include: ocriplasmin vitreolysis, pneumatic vitreolysis or vitrectomy.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.