13 Rhegmatogenous Retinal Detachment Special Scenarios
13.1 Rhegmatogenous Retinal Detachment: Re-detachment Surgery
13.2 Macular Hole Retinal Detachment
13.3 Retinoschisis Detachment
13.4 Optic Disc Pit Retinal Detachment and Maculopathy
13.5 Giant Retinal Tear Detachment
13.6 Retinal Dialysis
13.7 Macular Folds
13.8 Sickle Cell Detachment
13.9 Viral Retinitis Associated Retinal Detachment
13.10 Paediatric Retinal Detachment
13.8 Sickle Cell Detachment
Patients with sickle cell anemia, including genotype Hb SS and Hb SC, and S Thalassemia develop ocular manifestations of sickle cell disease. Both anterior and posterior segments of the eye can be affected by microvascular occlusions. Sickle cell retinopathy (SCR) is triggered by repeated episodes of vaso-occlusion of the microvasculature, leading to a spectrum of retinal manifestations from nonproliferative to proliferative sickle cell retinopathy (PSR). Clinical features of nonproliferative SCR include salmon patch hemorrhages, iridescent spots and black sunbursts, enlargement of the foveal avascular zone, and angioid streaks. In PSR, peripheral retinal neovascularization develops due to chronic ischemia of peripheral retina and is characterized initially by flat sea fan vessels.[1] Sea fan neovascular complexes grow anteriorly from perfused to non-perfused retina and can lead to sight-threatening complications, including vitreous hemorrhage, vitreo-retinal traction, and rhegmatogenous and/or combined rhegmatogenous tractional retinal detachment (Figure 13.8.1). Indications for vitreoretinal surgery in PSR include removal of non-clearing sight-threatening vitreous hemorrhage, repair of retinal detachment, and less commonly, to address the complications of vitreomacular interface abnormalities such as macular hole, vitreomacular traction, or epiretinal membrane.
Scott AW: Ophthalmic Manifestations of Sickle Cell Disease. South Med J 109:542-548, 2016
Figure 13.8.1
49-year-old female with proliferative sickle retinopathy and regressed sea fan neovascularization in the inferotemporal quadrant of the right eye that was previously treated with scatter laser photocoagulation presented with a fovea-sparring combined tractional/rhegmatogenous retinal detachment with atrophic retina from 4 to 10 o’clock (A, B). She underwent 23-gauge pars plana vitrectomy and a causative break was identified at the base of regressed sea-fan (A, arrow). The seafan neovascular complex was gently lifted from the retinal surface with the cutter to relieve traction and the retina was flattened with gas tamponade. At 4-month post-operative follow-up, the retina was attached and a demarcation line in the inferior macula was evident (C, D).
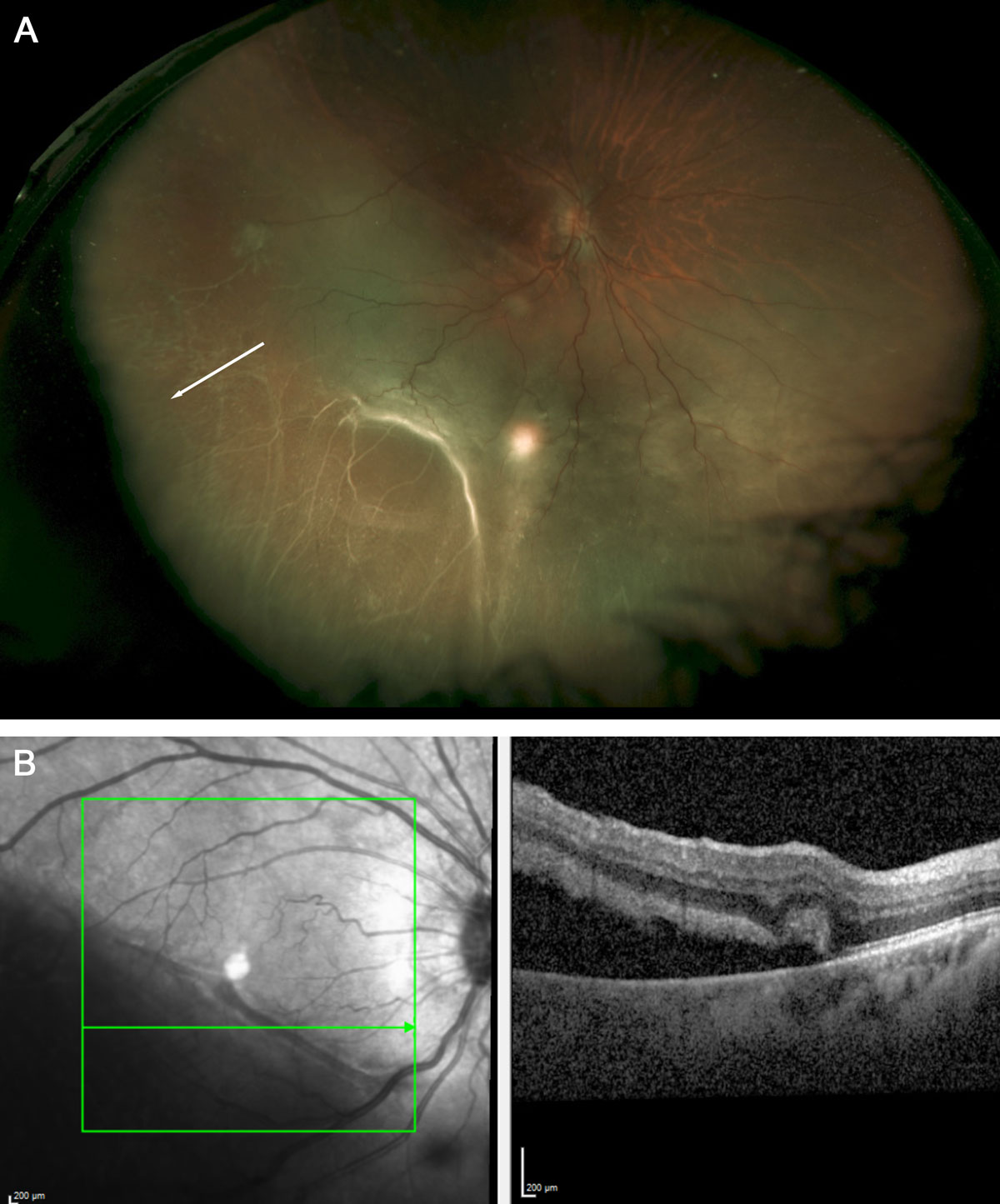
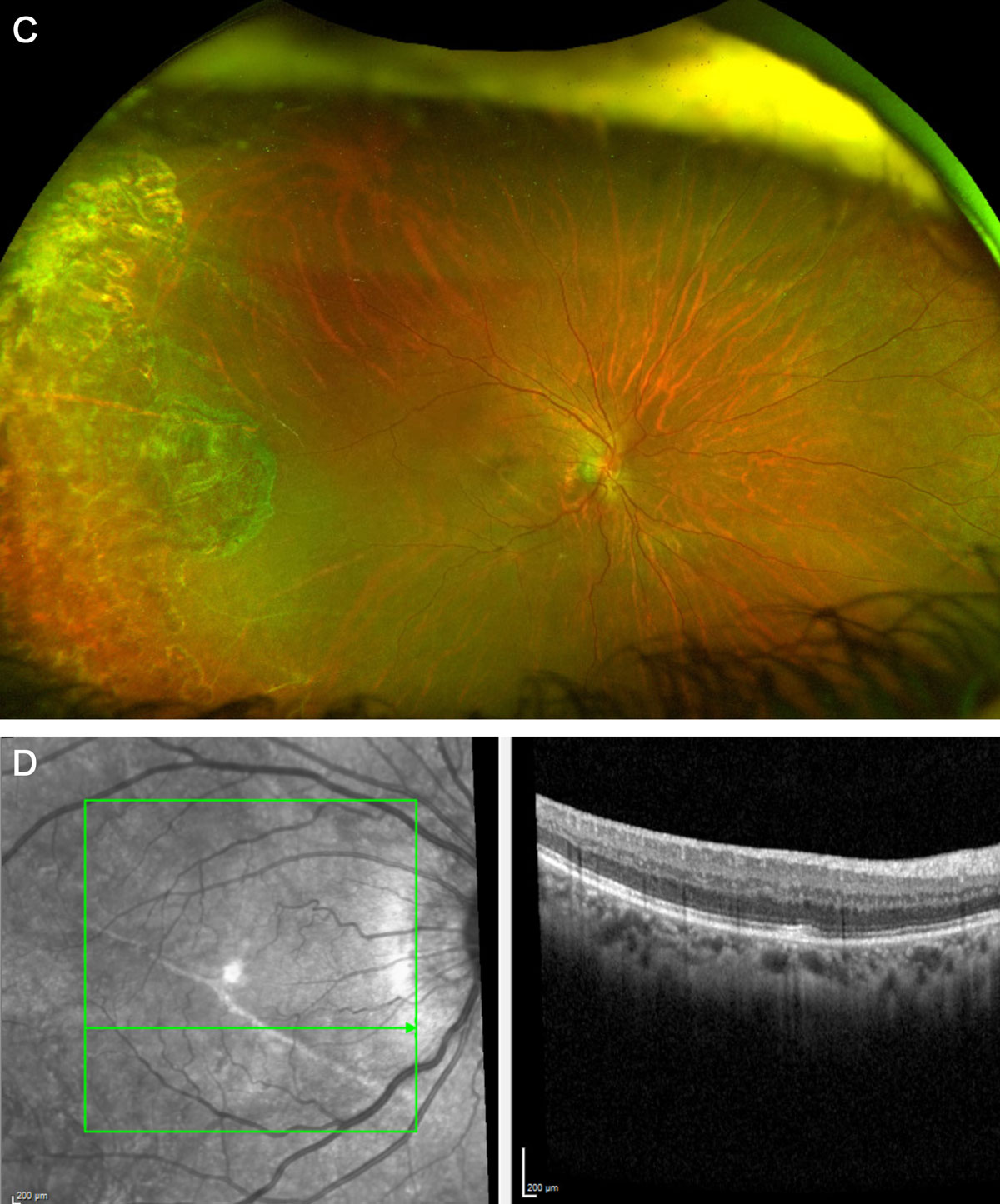
Figure 13.8.1
49-year-old female with proliferative sickle retinopathy and regressed sea fan neovascularization in the inferotemporal quadrant of the right eye that was previously treated with scatter laser photocoagulation presented with a fovea-sparring combined tractional/rhegmatogenous retinal detachment with atrophic retina from 4 to 10 o’clock (A, B). She underwent 23-gauge pars plana vitrectomy and a causative break was identified at the base of regressed sea-fan (A, arrow). The seafan neovascular complex was gently lifted from the retinal surface with the cutter to relieve traction and the retina was flattened with gas tamponade. At 4-month post-operative follow-up, the retina was attached and a demarcation line in the inferior macula was evident (C, D).
Perioperative Planning
Sickle cell disease is a systemic process and affects every organ system. Unlike other ocular surgeries, a multidisciplinary approach to preoperative planning among the vitreoretinal surgeon, anesthesiologist, and the hematologist is essential. Preoperative blood exchange transfusion to raise Hb A levels to more than 60% may be considered to decrease risk for anterior ischemia[2] and to potentially decrease likelihood of systemic vaso-occlusive pain crises in the peri-operative period. However, there is no clear evidence in either the hematology or ophthalmology literature on the benefit of preoperative blood transfusion and such decisions should be tailored to the individual’s medical history and in consultation with hematologist.[3,4] Efforts to minimize postoperative pain are also imperative because poor postoperative hydration, analgesia and stress of surgery can trigger a positive feedback loop of vaso-occlusive pain crisis.
Vitreous hemorrhage in PSR may often be managed clinically with observation and scatter laser photocoagulation if the view of the posterior segment allows. Intravitreal bevacizumab has been reported to be a helpful adjunct to scatter laser treatment in PSR to facilitate clearing of vitreous hemorrhage, and avoiding the potential morbidity of vitreoretinal surgery for these patients.[5]
Howard J, Malfroy M, Llewelyn C, et al.: The Transfusion Alternatives Preoperatively in Sickle Cell Disease (TAPS) study: a randomised, controlled, multicentre clinical trial. Lancet 381:930-938, 2013
Estcourt LJ, Fortin PM, Trivella M, Hopewell S: Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev 4:CD003149, 2016
Pulido JS, Flynn HW, Jr., Clarkson JG, Blankenship GW: Pars plana vitrectomy in the management of complications of proliferative sickle retinopathy. Arch Ophthalmol 106:1553-1557, 1988
Cai CX, Linz MO, Scott AW: Intravitreal Bevacizumab for Proliferative Sickle Retinopathy: A Case Series. Journal of VitreoRetinal Diseases 2:32-38, 2018
Surgical Considerations
Intraoperative analgesia, oxygenation, and hydration are essential during surgery for sickle cell disease patients. General anesthesia is preferred over local anesthesia in these patients and, if general anesthesia is contraindicated, sub-Tenons block is preferred over retrobulbar block due to theoretical increased risk of orbital compartment syndrome from sickling events associated with a retrobulbar block. Topical or systemic acetazolamide should be avoided.
The goals of surgery in PSR retinal detachment repair are similar to any other retinal detachment repair – to clear media opacity, relieve vitreoretinal traction, and treat all breaks. Preoperative intravitreal bevacizumab (days to weeks prior to surgery) can be a useful adjunct to decrease the likelihood of intraoperative bleeding and to facilitate dissection of sea fan membranes.[6]
Patients with PSR tend to be younger, phakic, and have a formed vitreous. The use of encircling scleral buckle was previously discouraged, citing risk of anterior segment ischemia.[7] However, with modern surgical techniques and care taken to avoid placing a high and broad buckle, encircling scleral buckle elements can adequately support the vitreous base without compromising perfusion of the anterior choroid and ciliary body.[8]
Relieving vitreoretinal traction associated with neovascular membranes can be accomplished via either segmentation and/or delamination techniques. Bi-manual approach with a chandelier light or lighted pick can greatly facilitate dissection. Segmentation involves the vertical cutting of fibrovascular tissue into small segments to relieve anterior-posterior traction, whereas, delamination involves removal of membranes through horizontal dissection in the plane between retina and fibrous tissue to remove tangential traction. Some surgeons advocate for segmentation over delamination since delamination carries a higher risk of iatrogenic breaks in the already thin, atrophic peripheral retina. The sea fan neovascular complexes are also usually firmly adherent to underlying retina and removing them by delamination can be challenging.[9] Endolaser is performed to treat all retinal breaks, to surround and barricade neovascular complexes, and may be added to peripheral non-perfused retina to ablate ischemic retina, in efforts to decrease further vascular endothelial growth factor drive. Care must be taken to prevent intraocular pressure elevation during surgery, and also at the close of surgery with placement of gas or silicone oil tamponade. Eyes with SCR are prone to vitreoschisis and prudent use of dilute Kenalog is advised to ensure that a full posterior vitreous detachment is induced. PFO can be used to stabilize bullous retina and to aid in elevation of sticky peripheral hyaloid. Occasionally, removal of the crystalline lens may be needed to accomplish goals in the periphery.
The surgical outcomes in PSR are generally good when surgery is performed for vitreous hemorrhage or epiretinal membrane. In a case series of 15 patients with PSR, 6 patients with vitreous hemorrhage and 1 with ERM, underwent PPV and all had improved vision postoperatively.[8] The prognosis for PSR-related retinal detachment is more guarded. In the same case series, 4 of 8 patients with retinal detachment developed recurrent detachment (50% primary reattachment rate). In a separate retrospective case series that included 38 eyes with retinal detachment, the primary reattachment rate was 79%. Both studies highlight the complexity of treating retinal detachment in patients with proliferative sickle retinopathy.[10]
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.
Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.